Opioid use disorder (OUD) during pregnancy presents significant risks to both maternal and fetal health, including complications such as preterm birth, low birth weight, and overdose. As a result, pharmacotherapy—primarily with medications like methadone and buprenorphine—has become the standard of care for managing OUD in pregnant individuals. Rather than attempting abrupt cessation of opioid use, which can lead to harmful withdrawal effects, these medications help stabilize brain function, reduce cravings, and support consistent prenatal care. Understanding the role of pharmacotherapy is essential for promoting safer pregnancies and improving outcomes for both mother and child.
Supporting Two Lives: Pharmacotherapy for Opioid Use Disorder in Pregnancy
Opioid use disorder (OUD) during pregnancy presents a complex clinical and public health challenge, affecting both maternal health and fetal development. Untreated OUD is associated with serious risks, including preterm birth, low birth weight, and overdose. As a result, pharmacotherapy—particularly opioid agonist treatment—is considered the standard of care for pregnant individuals with OUD. Rather than discontinuing opioid use abruptly, which can be dangerous, evidence-based medications help stabilize both the mother and the developing fetus.
What Is Pharmacotherapy in Pregnancy?
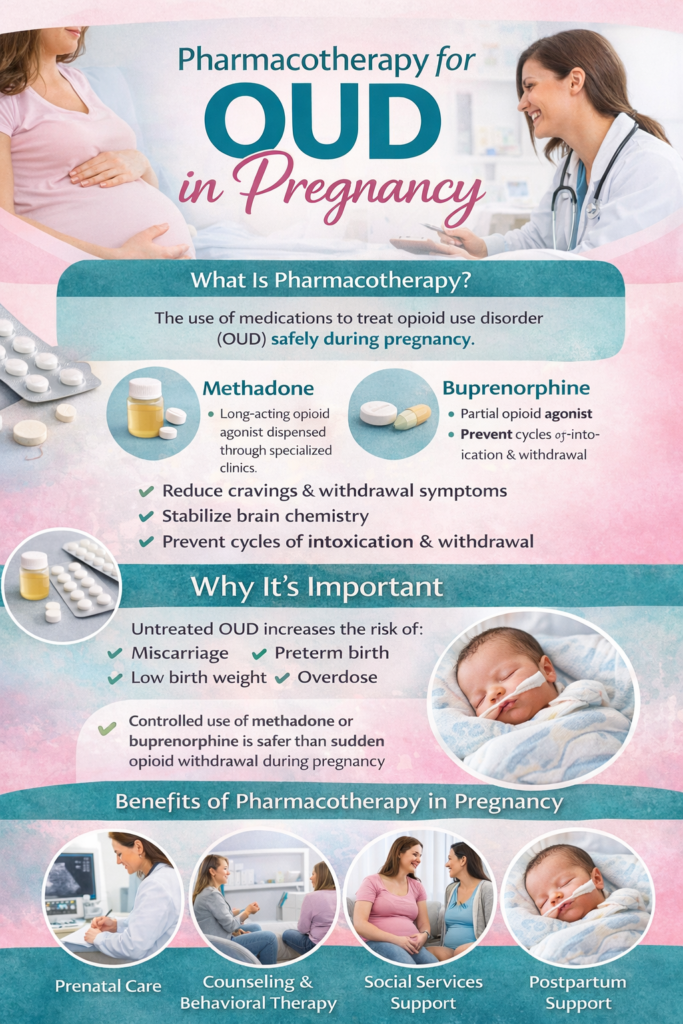
Pharmacotherapy refers to the use of medications to treat OUD. The two most commonly used medications during pregnancy are:
- Methadone – a long-acting opioid agonist dispensed through specialized clinics
- Buprenorphine – a partial opioid agonist that can often be prescribed in outpatient settings
Both medications work by:
- Reducing cravings and withdrawal symptoms
- Stabilizing brain chemistry
- Preventing cycles of intoxication and withdrawal
This stability is critical for maintaining a healthy pregnancy.
Why Pharmacotherapy Is Recommended
Stopping opioid use suddenly during pregnancy can lead to withdrawal, which may increase the risk of miscarriage or preterm labor. Pharmacotherapy helps avoid these risks by providing a controlled, consistent level of medication.
Benefits include:
- Improved prenatal care engagement
- Reduced risk of relapse and overdose
- Better maternal stability and functioning
- Improved fetal growth and outcomes
Methadone vs. Buprenorphine in Pregnancy
Both medications are effective, but they have some differences:
- Methadone
- Requires daily clinic visits
- Long history of use in pregnancy
- May be associated with more structured care
- Buprenorphine
- Can often be prescribed in office-based settings
- Lower risk of severe neonatal abstinence syndrome (NAS) in some studies
- Greater flexibility for some patients
The choice depends on individual factors such as access, medical history, and treatment response.
Neonatal Abstinence Syndrome (NAS)
One important consideration is neonatal abstinence syndrome (NAS), a condition where newborns experience withdrawal after birth.
Key points:
- NAS is expected and treatable
- Symptoms may include irritability, feeding difficulties, and tremors
- Hospitals are equipped to monitor and manage NAS safely
Importantly, the benefits of pharmacotherapy outweigh the risks of untreated OUD, even when NAS occurs.
The Role of Comprehensive Care
Medication alone is not enough. Effective treatment includes:
- Prenatal care
- Behavioral therapy or counseling
- Social and community support
- Postpartum follow-up care
This integrated approach supports both maternal recovery and infant health.
Postpartum Considerations
The postpartum period is a high-risk time for relapse and overdose. Continued pharmacotherapy is often recommended to:
- Maintain stability
- Support parenting and bonding
- Reduce overdose risk
Breastfeeding is often encouraged for individuals on methadone or buprenorphine when medically appropriate, as it can benefit both mother and baby.
Addressing Stigma and Barriers
Pregnant individuals with OUD often face stigma, which can discourage them from seeking care. It is essential to recognize that:
- OUD is a medical condition, not a moral failure
- Pharmacotherapy is evidence-based and life-saving
- Compassionate, nonjudgmental care improves outcomes
Reducing stigma helps ensure that more individuals receive the treatment they need.
Final Thoughts
Pharmacotherapy for opioid use disorder during pregnancy is a critical component of modern maternal healthcare. By stabilizing the mother and supporting fetal development, medications like methadone and buprenorphine provide a safer pathway for both lives.
When combined with comprehensive care and ongoing support, pharmacotherapy offers not just treatment—but the foundation for healthier pregnancies, safer deliveries, and stronger starts for both mother and child.
Taking Control of Care: Self-Management Strategies for Understanding Pharmacotherapy for OUD in Pregnancy
Managing opioid use disorder (OUD) during pregnancy can feel overwhelming, especially when navigating treatment options like methadone or buprenorphine. Pharmacotherapy is a safe and evidence-based approach that helps stabilize both the mother and developing baby—but understanding how to actively engage in treatment is just as important as the medication itself.
Self-management strategies empower pregnant individuals to take an active role in their care, improve treatment outcomes, and build confidence throughout pregnancy and beyond.
Why Self-Management Matters During Pregnancy
Pregnancy is a time of increased physical, emotional, and medical needs. When combined with OUD treatment, it requires:
- Consistent medical care
- Careful monitoring of symptoms
- Strong communication with providers
Self-management helps individuals:
- Stay engaged in treatment
- Recognize changes in their body
- Advocate for their needs
- Reduce stress and uncertainty
Understanding Pharmacotherapy Basics
Pharmacotherapy for OUD typically includes:
- Methadone (clinic-based, structured care)
- Buprenorphine (often office-based, more flexible)
Both medications:
- Reduce cravings and withdrawal
- Help maintain stability
- Support healthier pregnancy outcomes
Understanding how your medication works can reduce fear and increase confidence.
Key Self-Management Strategies
1. 📘 Educate Yourself About Your Treatment
Knowledge is empowering. Learn:
- How your medication affects your body and pregnancy
- Expected benefits and possible side effects
- What to expect during prenatal visits and delivery
Ask questions and keep notes—you deserve to understand your care.
2. 📅 Stay Consistent with Medication and Appointments
Consistency is critical for both maternal and fetal health.
Try to:
- Take medication exactly as prescribed
- Attend all prenatal and treatment appointments
- Set reminders or use a planner
Missing doses or visits can increase risks for both you and your baby.
3. 📊 Monitor Your Physical and Emotional Health
Track:
- Cravings or withdrawal symptoms
- Mood changes (anxiety, depression)
- Sleep and energy levels
- Physical symptoms
This helps you notice patterns and share important information with your provider.
4. 🗣️ Communicate Openly with Your Healthcare Team
Your care team is there to support—not judge—you. Be honest about:
- Medication effects
- Challenges or concerns
- Substance use or cravings
Open communication allows for better, safer treatment adjustments.
5. 🧘 Practice Stress Management and Coping Skills
Stress can increase cravings and impact pregnancy. Helpful strategies include:
- Deep breathing or mindfulness
- Prenatal yoga or light exercise
- Journaling or talking to a counselor
These tools support both mental health and recovery.
6. 🤝 Build a Support System
Self-management doesn’t mean doing everything alone. Seek support from:
- Family or trusted friends
- Support groups for pregnant individuals in recovery
- Counselors or case managers
Support improves accountability and emotional well-being.
7. ⚖️ Prepare for Postpartum Care
Recovery continues after delivery. Plan ahead by:
- Discussing postpartum treatment with your provider
- Arranging follow-up appointments
- Identifying support for childcare and recovery
The postpartum period is a critical time for maintaining stability.
Challenges to Expect
Even with strong self-management:
- Hormonal and emotional changes can be intense
- Stigma or fear may arise
- Adjusting to medication may take time
These challenges are normal and manageable with support.
The Bigger Picture: Empowered Pregnancy and Recovery
Pharmacotherapy provides the medical foundation—but self-management builds the structure for long-term success. When individuals are informed, consistent, and engaged, they improve outcomes for both themselves and their babies.
Final Thoughts
You are not just receiving treatment—you are actively shaping your health and your child’s future. By learning, tracking, communicating, and seeking support, you can navigate pharmacotherapy with confidence and care.
Recovery during pregnancy is not only possible—it is a powerful step toward a healthier life for both mother and child.
Supporting Mother and Baby: Family Strategies for Understanding Pharmacotherapy for OUD in Pregnancy
When a loved one is pregnant and receiving treatment for opioid use disorder (OUD), families often experience a mix of concern, confusion, and a strong desire to help. Medications like methadone and buprenorphine are evidence-based treatments that support both maternal health and fetal development—but misunderstandings and stigma can make it difficult for families to fully embrace these approaches.
Family support plays a critical role in helping pregnant individuals stay engaged in treatment, reduce stress, and build a healthy foundation for both mother and baby. By understanding pharmacotherapy and adopting supportive strategies, families can become an essential part of the recovery journey.
Why Family Understanding Matters
Pharmacotherapy during pregnancy is often misunderstood. Some families may worry that medication could harm the baby or “replace one addiction with another.” In reality:
- These treatments are medically supervised and evidence-based
- They reduce risks compared to untreated OUD
- They help stabilize both the mother and the developing fetus
When families understand this, they are more likely to respond with support rather than fear or judgment.
Key Family Support Strategies
1. 📘 Educate Yourself About OUD and Treatment
Learning the basics can reduce stigma and confusion. Take time to understand:
- How methadone and buprenorphine work
- Why is pharmacotherapy recommended during pregnancy
- What to expect during prenatal care and delivery
Accurate knowledge helps families provide informed, compassionate support.
2. 🗣️ Communicate with Empathy and Respect
Pregnancy and recovery can both be emotionally challenging. Supportive communication includes:
- Listening without judgment or criticism
- Avoiding blame or shame
- Asking how you can help instead of making assumptions
For example:
Instead of “Why are you still on medication?”
Try “How can I support you during your treatment?”
3. 🚗 Support Consistency in Treatment
Consistency is essential for both recovery and pregnancy health. Families can help by:
- Providing transportation to appointments or clinics
- Helping manage schedules and reminders
- Encouraging adherence to medication plans
Reliable support can reduce stress and improve outcomes.
4. 🏡 Create a Safe and Stable Environment
A calm and supportive home environment benefits both mother and baby. Families can:
- Reduce conflict and stress
- Encourage healthy routines (sleep, meals, structure)
- Provide emotional reassurance
Stability reinforces the effectiveness of treatment.
5. 🤝 Encourage Holistic Care
Medication is only one part of care. Families can encourage:
- Prenatal care visits
- Counseling or therapy
- Support groups for pregnant individuals in recovery
- Healthy lifestyle habits
This comprehensive approach supports long-term recovery.
6. ⚖️ Set Healthy Boundaries
Support does not mean ignoring challenges. Families should:
- Set clear, respectful boundaries
- Avoid enabling harmful behaviors
- Take care of their own well-being
Healthy boundaries create balance between support and accountability.
Understanding Neonatal Abstinence Syndrome (NAS)
Families should also be aware of neonatal abstinence syndrome (NAS):
- It is a treatable condition where newborns may experience withdrawal
- It is expected with opioid agonist therapy
- Medical teams are trained to manage it safely
Understanding NAS can reduce fear and help families stay focused on overall positive outcomes.
Challenges Families May Face
Supporting a pregnant loved one in recovery can be complex:
- Emotional stress and worry about the baby
- Misunderstandings about treatment
- Stigma from others
Seeking support—such as counseling or family groups—can help families stay strong and informed.
The Bigger Picture: Supporting Two Lives
Pharmacotherapy during pregnancy is about protecting both the mother and the child. Family support strengthens this process by providing stability, encouragement, and understanding.
Final Thoughts
You don’t have to be a medical expert to make a difference. By learning, listening, and showing consistent support, families can help create a healthier, safer path for both mother and baby.
Recovery during pregnancy is not just an individual journey—it’s a shared effort built on compassion, knowledge, and support.
Community Care for Two: Resource Strategies for Understanding Pharmacotherapy for OUD in Pregnancy
Opioid use disorder (OUD) during pregnancy is a complex health issue that requires coordinated care, compassion, and access to reliable resources. While pharmacotherapy—including medications like methadone and buprenorphine—is the standard of care, many individuals and families face challenges in understanding, accessing, and maintaining treatment. This is where community resources become essential.
Communities play a powerful role in supporting pregnant individuals with OUD by improving education, reducing stigma, and connecting people to the care they need for both maternal and infant health.
Why Community Resources Matter
Pharmacotherapy during pregnancy can be misunderstood or stigmatized, leading to barriers in care. Community resources help by:
- Providing accurate, evidence-based information
- Increasing access to prenatal and addiction treatment services
- Supporting continuity of care before and after birth
- Creating supportive, nonjudgmental environments
These efforts improve outcomes for both mother and baby.
Key Community Resource Strategies
1. 🏥 Expand Access to Integrated Care Services
Communities can support programs that combine:
- Prenatal care
- Addiction treatment (methadone or buprenorphine)
- Mental health services
Integrated care reduces fragmentation and ensures that individuals receive comprehensive, coordinated support in one setting.
2. 📢 Promote Public Education and Awareness
Education helps reduce fear and stigma. Community efforts may include:
- Workshops or seminars on OUD in pregnancy
- Outreach campaigns explaining pharmacotherapy
- Educational materials in clinics and community centers
Clear messaging reinforces that pharmacotherapy is safe, effective, and recommended.
3. 🚍 Address Transportation and Access Barriers
Accessing consistent care can be difficult, especially when:
- Methadone requires daily clinic visits
- Prenatal appointments are frequent
Communities can help by offering:
- Transportation services or vouchers
- Mobile health units
- Telehealth support when appropriate
Reducing barriers improves treatment adherence and outcomes.
4. 🤝 Provide Peer Support and Parenting Resources
Peer programs connect individuals with others who have lived experience. These programs:
- Offer emotional support and encouragement
- Help normalize treatment participation
- Provide guidance on parenting and recovery
Support from peers can be especially powerful during pregnancy and the postpartum period.
5. 📋 Offer Case Management and Care Navigation
Navigating healthcare systems can be overwhelming. Community-based case managers can assist with:
- Scheduling appointments
- Coordinating prenatal and addiction care
- Understanding insurance and coverage
- Connecting to housing, nutrition, and social services
This support ensures that individuals do not fall through the cracks in care.
6. 🏫 Reduce Stigma Through Community Engagement
Stigma is one of the biggest barriers to treatment. Communities can:
- Promote OUD as a medical condition
- Encourage compassionate, nonjudgmental care
- Share recovery success stories
Reducing stigma makes individuals more likely to seek and stay in treatment.
Challenges to Consider
Despite strong community efforts, challenges remain:
- Limited availability of specialized programs
- Variability in insurance coverage
- Lack of awareness among providers and the public
- Persistent stigma
Addressing these challenges requires ongoing advocacy and collaboration.
The Bigger Picture: Community as a Foundation for Healthy Outcomes
Pharmacotherapy provides the medical foundation for treating OUD in pregnancy—but community resources build the support system that makes treatment accessible and sustainable. When communities invest in education, access, and support, they improve outcomes not just for individuals, but for families and future generations.
Final Thoughts
Supporting pregnant individuals with OUD is about more than treatment—it’s about connection, compassion, and community. By strengthening community resources, we can help ensure that pharmacotherapy is understood, accessible, and effective.
Healthy mothers, healthy babies, and stronger communities all begin with informed and supportive care.
Frequently Asked Questions
Here are some common questions:
1. What is pharmacotherapy for OUD in pregnancy?
Answer:
Pharmacotherapy refers to the use of medications—primarily methadone or buprenorphine—to treat opioid use disorder during pregnancy. These medications help stabilize the mother and support healthier outcomes for the baby.
2. Why is medication recommended instead of stopping opioids completely?
Answer:
Stopping opioids suddenly can cause withdrawal, which may lead to:
- Miscarriage
- Preterm labor
- Fetal distress
Pharmacotherapy provides a controlled, stable alternative that reduces these risks.
3. What medications are commonly used?
Answer:
The two main medications are:
- Methadone – dispensed through specialized clinics
- Buprenorphine – often prescribed in office-based settings
Both are considered safe and effective during pregnancy.
4. Are these medications safe for the baby?
Answer:
Yes. While no medication is completely risk-free, methadone and buprenorphine are the safest options compared to untreated OUD. They improve overall pregnancy outcomes.
5. What is neonatal abstinence syndrome (NAS)?
Answer:
NAS is a condition where newborns experience withdrawal after birth due to exposure to opioids in utero. Symptoms may include:
- Irritability
- Feeding difficulties
- Tremors
NAS is expected to be manageable and treatable in a hospital setting.
6. Is NAS dangerous?
Answer:
NAS can be uncomfortable for the baby, but it is rarely life-threatening when properly treated. Medical teams monitor and manage symptoms carefully.
7. Can I breastfeed while on methadone or buprenorphine?
Answer:
In most cases, yes. Breastfeeding is often encouraged because it:
- Supports bonding
- May help reduce NAS severity
Always consult your healthcare provider.
8. Will I need to take medication throughout pregnancy?
Answer:
Yes, most individuals remain on medication throughout pregnancy to maintain stability. Adjustments may be made as needed by a healthcare provider.
9. Can I stop medication after giving birth?
Answer:
Not immediately. The postpartum period is a high-risk time for relapse and overdose, so continuing medication is often recommended.
10. What are the side effects of methadone and buprenorphine?
Answer:
Common side effects include:
- Constipation
- Drowsiness
- Nausea
These are generally manageable and monitored by providers.
11. Is one medication better than the other?
Answer:
Both are effective.
- Methadone may offer more structure
- Buprenorphine may have fewer severe NAS symptoms in some cases
The best choice depends on individual needs.
12. Do I have to go to a clinic every day?
Answer:
- Methadone: Often requires daily clinic visits (especially early in treatment)
- Buprenorphine: Usually allows for more flexible prescriptions
13. Is pharmacotherapy just replacing one addiction with another?
Answer:
No. These medications:
- Are taken under medical supervision
- Do not produce the same harmful highs and lows
- Help restore normal functioning
They are treatment, not a substitution for addiction.
14. What other care is needed besides medication?
Answer:
Comprehensive care includes:
- Prenatal care
- Counseling or therapy
- Social and community support
- Postpartum follow-up
15. What happens during delivery?
Answer:
Healthcare providers will:
- Continue your medication
- Monitor both mother and baby
- Prepare to manage NAS if needed
A coordinated care plan helps ensure safety.
16. What are the risks of not receiving treatment?
Answer:
Untreated OUD increases the risk of:
- Overdose
- Poor prenatal care
- Preterm birth
- Low birth weight
Treatment significantly reduces these risks.
17. Will I be judged for being on medication during pregnancy?
Answer:
Unfortunately, stigma exists—but medically, pharmacotherapy is the recommended standard of care. Healthcare providers are trained to support, not judge.
18. How can I get started with treatment?
Answer:
You can:
- Talk to a healthcare provider or OB-GYN
- Contact addiction treatment programs
- Reach out to community health clinics
Early treatment leads to better outcomes.
Conclusion
Pharmacotherapy for OUD in pregnancy plays a critical role in protecting maternal health and supporting healthy fetal development. By reducing withdrawal symptoms and stabilizing opioid use, medications such as methadone and buprenorphine provide a safer alternative to untreated addiction. While challenges such as stigma, access to care, and neonatal abstinence syndrome remain, the benefits of evidence-based treatment far outweigh the risks. When combined with comprehensive prenatal care, counseling, and community support, pharmacotherapy offers a pathway to healthier pregnancies, safer deliveries, and improved long-term outcomes for both mother and baby.
Video: