Repurposing existing drugs for addiction offers faster, low-cost treatment options but faces challenges like limited evidence, safety risks, low industry interest, and ethical concerns. Government agencies help guide regulation, research, and access.
Repurposed Medications for Addiction Treatment
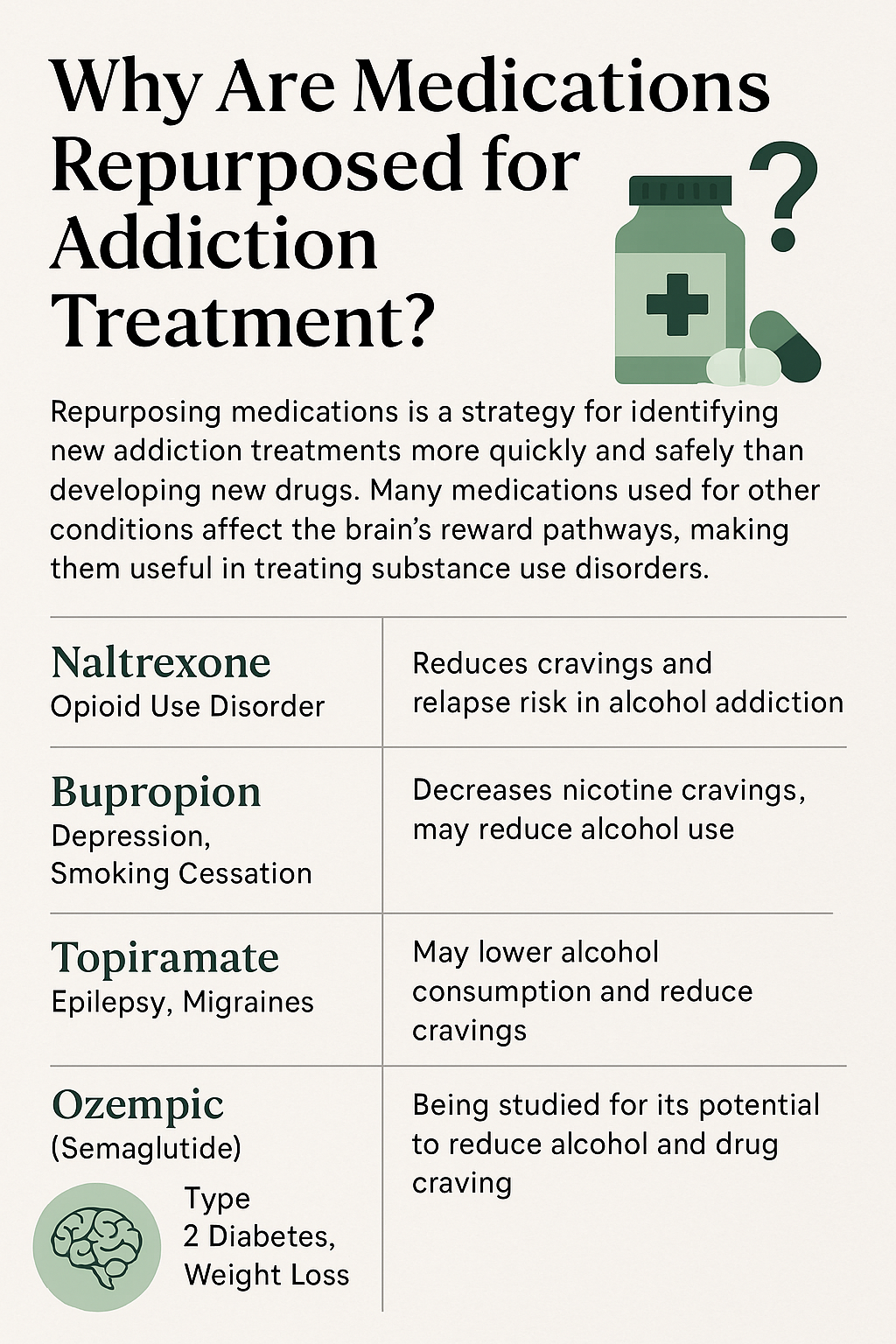
Repurposing existing medications—initially developed for other health conditions—is a promising and efficient strategy in addiction treatment. Since many of these drugs already have well-documented safety profiles, researchers can more quickly investigate their use in managing substance use disorders (SUDs). Below is a curated list of medications being studied or used off-label in addiction medicine:
1. Naltrexone
- Originally for: Alcohol dependence, opioid use disorder
- Now also used for:
- Methamphetamine use disorder (in combination with bupropion)
- Off-label for impulse control and behavioral addictions
2. Bupropion (Wellbutrin)
- Originally for: Depression, smoking cessation
- Repurposed for:
- Methamphetamine addiction (combined with naltrexone)
- Cocaine use disorder (in clinical trials)
3. Topiramate (Topamax)
- Originally for: Epilepsy, migraines
- Repurposed for:
- Alcohol use disorder
- Cocaine addiction (with mixed trial outcomes)
4. Gabapentin
- Originally for: Seizures, nerve pain
- Repurposed for:
- Alcohol withdrawal and relapse prevention
- Studied for opioid withdrawal support
5. Modafinil
- Originally for: Narcolepsy, ADHD
- Repurposed for:
- Cocaine and methamphetamine addiction (to support cognition and reduce cravings)
6. Ondansetron (Zofran)
- Originally for: Nausea/vomiting (especially in chemotherapy)
- Repurposed for:
- Alcohol dependence, especially in early-onset cases
7. Clonidine / Lofexidine
- Originally for: High blood pressure
- Repurposed for:
- Opioid withdrawal symptom relief
8. Ketamine
- Originally for: Anesthesia
- Repurposed for:
- Alcohol and opioid use disorders (experimental, helps with cravings and depression)
- Studied for relapse prevention and treatment-resistant depression in SUD patients
9. N-acetylcysteine (NAC)
- Originally for: Acetaminophen overdose, mucus clearance
- Repurposed for:
- Cocaine, cannabis, and nicotine addiction (modulate glutamate transmission)
10. Varenicline (Chantix)
- Originally for: Smoking cessation
- Repurposed for:
- Alcohol use disorder (reduces drinking and cravings)
- Investigated for stimulant use disorders
⚠️ Important Notes
- Many of these medications are used off-label or remain in clinical trial stages and are not yet FDA-approved for specific SUDs.
- Effectiveness varies by individual biology, substance type, and co-occurring mental health conditions.
- Always seek clinical supervision before starting or repurposing any medication.
Unique Challenges in Repurposing Drugs for Addiction Treatment
Repurposing existing drugs for addiction treatment holds promise—but also brings unique scientific, regulatory, and practical challenges that distinguish it from traditional drug development. Here are the key challenges:
1. 🔬 Mismatch Between Original Use and Addiction Biology
- Drugs may not fully address the complex neurobiology of addiction (e.g., craving, reward circuitry, withdrawal).
- Effects on neurotransmitters (e.g., dopamine, glutamate) may differ significantly when used for addiction versus the original condition.
2. 🧪 Lack of Robust Efficacy Data
- Initial studies often show inconsistent or marginal effects, especially in real-world settings.
- Placebo effects in addiction trials can be strong, making it harder to demonstrate statistical significance.
- Most repurposing studies are small-scale or preliminary, limiting confidence in outcomes.
3. 🧠 Patient Heterogeneity
- People with addiction often have co-occurring mental health or medical conditions that complicate treatment.
- A medication that works in one substance use disorder (SUD) population may not work in another (e.g., cocaine vs. alcohol).
4. 🧾 Regulatory and Funding Barriers
- Lack of commercial incentive for pharmaceutical companies—patents may have expired, or profit margins are low.
- Securing FDA approval for a new indication can be expensive and time-consuming.
- Government and academic funding for repurposing SUD medications is limited and highly competitive.
5. 💊 Stigma and Perception
- Stigma surrounding addiction may lead to skepticism about using medications—even among clinicians.
- Patients may be reluctant to use a drug associated with another condition (e.g., antiepileptics, antidepressants).
6. 📉 Adherence and Abuse Potential
- Some repurposed medications (e.g., gabapentin, bupropion) carry a risk of misuse, especially in vulnerable populations.
- Side effects from the original use (e.g., cognitive dulling, sedation) can affect adherence in people with addiction.
7. 📊 Outcome Measurement and Trial Design
- Addiction outcomes are often complex and multidimensional (e.g., cravings, relapse, functioning).
- Difficult to define “success” in trials—abstinence vs. harm reduction, frequency vs. severity of use.
In summary, repurposing drugs for addiction treatment is an innovative and resource-efficient strategy, but it requires careful consideration of scientific fit, regulatory strategy, patient variability, and practical implementation hurdles. Overcoming these challenges demands strong clinical trial design, interdisciplinary collaboration, and sustained advocacy to expand access and acceptance.
Challenges in Repurposing Medications for Addiction Treatment
Repurposing existing drugs for addiction treatment holds tremendous promise—but also presents distinct scientific, regulatory, and clinical challenges that differ significantly from traditional drug development pathways. Below are the significant barriers researchers and clinicians must navigate:
1. 🔬 Mismatch Between Original Use and Addiction Neurobiology
- Repurposed drugs may not adequately target the complex neural mechanisms involved in addiction—such as craving, reward, and withdrawal.
- Neurotransmitter effects (e.g., on dopamine, glutamate) may vary when drugs are used for addiction versus their original indication.
2. 🧪 Lack of Robust Efficacy Data
- Early studies often show modest or inconsistent results, especially in real-world settings.
- Strong placebo effects in addiction trials can mask actual drug impact.
- Most studies are small-scale or preliminary, limiting the strength of evidence and confidence in clinical utility.
3. 🧠 Patient Heterogeneity
- People with substance use disorders (SUDs) often have co-occurring mental health and medical conditions, complicating treatment.
- Medications may not generalize well across different addiction types (e.g., alcohol vs. stimulants).
4. 🧾 Regulatory and Funding Barriers
- Low commercial interest due to expired patents or limited profitability.
- Gaining FDA approval for new addiction-related uses is costly and time-intensive.
- Public and academic funding for repurposing addiction medications is limited and highly competitive.
5. 💊 Stigma and Perception
- Stigma around addiction can lead to hesitation—even among providers—to use repurposed medications.
- Patients may be wary of drugs linked to other conditions (e.g., anti-seizure or psychiatric medications).
6. 📉 Adherence and Abuse Potential
- Some repurposed drugs (like gabapentin or bupropion) carry misuse or diversion risks.
- Side effects such as sedation or cognitive impairment may reduce medication adherence in this population.
7. 📊 Complexity in Outcome Measurement
- Addiction treatment outcomes are often multi-layered: reduced use, improved function, fewer cravings, and better quality of life.
- There is no universal definition of success—abstinence vs. harm reduction remains a debated endpoint in trials.
In summary, while repurposing medications for addiction treatment is cost-effective and innovative, it’s not without complications. Success depends on addressing key barriers: from scientific alignment and patient diversity to stigma and trial complexity. Advancing this approach will require stronger clinical trial designs, cross-disciplinary collaboration, and policy-level support to unlock new options for individuals struggling with addiction.
Navigating U.S. Regulations for Repurposed Drugs in Addiction Treatment
Repurposing medications for addiction care falls under a mix of federal laws, FDA pathways, and ethical clinical practices. While this strategy is innovative and cost-effective, it is often hindered by regulatory gray zones, particularly for addiction-specific applications where many drugs are used off-label.
⚖️ Key Regulatory Frameworks
1. FDA Approval Process
- The U.S. Food and Drug Administration (FDA) requires any new drug indication—even for previously approved drugs—to go through its formal approval process.
- To repurpose a medication for addiction, researchers or companies typically need to submit:
- An Investigational New Drug (IND) application to begin trials
- A New Drug Application (NDA) or Supplemental NDA (sNDA) for approval of the new use
- Most medications used for substance use disorders (SUDs) today are prescribed off-label, meaning they are not FDA-approved for addiction but can still be legally used under medical supervision.
2. Off-Label Prescribing Rules
- Off-label prescribing is legal and frequently used in addiction care.
- However:
- Drug manufacturers cannot promote medications for off-label addiction treatment.
- Clinicians must rely on evidence-based guidelines (e.g., ASAM or SAMHSA) and use best judgment.
3. Clinical Trial Oversight
- Any study repurposing drugs for addiction must adhere to:
- Institutional Review Board (IRB) oversight to protect human subjects
- FDA Good Clinical Practice (GCP) protocols
- Trials involving people with SUDs face additional ethical scrutiny due to their status as a potentially vulnerable population.
4. Controlled Substances Act (CSA)
- If the repurposed medication is a controlled substance (e.g., gabapentin or bupropion in some states), prescribers must:
- Be registered with the DEA
- Follow state-specific laws and dispensing limits
- Use tools like Prescription Drug Monitoring Programs (PDMPs) to track prescriptions
5. Medicaid & Medicare Coverage Rules
- Off-label prescriptions may not be covered by insurance, primarily Medicaid or Medicare, unless supported by solid evidence.
- Formulary decisions vary across states, and some addiction-specific uses may be excluded even when clinically appropriate.
6. HITECH, HIPAA & 42 CFR Part 2
- When used in addiction treatment settings, repurposed drugs are subject to federal privacy regulations, including:
- HIPAA (Health Insurance Portability and Accountability Act)
- 42 CFR Part 2, which imposes stricter confidentiality standards for substance use treatment records
7. NIH and NIDA Oversight
- The National Institute on Drug Abuse (NIDA) plays a leading role by funding trials and guiding national research priorities.
- Findings from NIDA-supported studies often shape clinical practice guidelines and influence policy.
🚨 Regulatory Gaps and Challenges
- No fast-track FDA pathway currently exists specifically for addiction repurposing efforts.
- Low commercial incentive discourages pharmaceutical companies from pursuing formal approval.
- Lack of regulatory clarity makes it difficult for clinicians to navigate off-label prescribing with confidence.
✅ Recommendations for Providers and Researchers
- Ground all prescribing decisions in peer-reviewed evidence and use guidance from ASAM, SAMHSA, or national consensus documents.
- Clearly inform patients when a drug is being used off-label and obtain informed consent when appropriate.
- Advocate for policy reform to increase funding, streamline approval, and promote insurance coverage parity for evidence-based repurposed treatments.
Frequently Asked Questions
Here are some common questions:
Question: Why are medications repurposed for addiction treatment?
Answer:
🔁 1. Faster Development and Approval
- Existing safety data: Repurposed drugs have already passed toxicity, safety, and pharmacokinetic trials.
- This speeds up research timelines compared to developing a new drug from scratch.
💰 2. Lower Cost
- Drug development is expensive and time-consuming. Repurposing avoids early-stage development costs.
- Generic drugs can be investigated for new uses without significant investments in manufacturing or marketing.
🧠 3. Potential Fit with Addiction Neurobiology
- Many existing drugs target neurotransmitter systems (e.g., dopamine, glutamate, serotonin) involved in addiction.
- Some medications developed for depression, seizures, or pain also reduce cravings, improve mood, or ease withdrawal symptoms.
🧪 4. Encouraging Early Evidence
- Pilot studies or case reports often reveal unexpected benefits for addiction-related symptoms.
- This can lead researchers to test these drugs in larger trials.
⚕️ 5. Limited FDA-Approved Options
- There are relatively few FDA-approved medications for substance use disorders, especially for stimulants and cannabis.
- Repurposing fills critical treatment gaps for underserved addictions.
🌍 6. Broader Access in Clinical Settings
Providers may feel more comfortable prescribing them off-label when they are familiar with the drug’s profile.
Repurposed drugs are often already stocked in hospitals and clinics.
Question: Who profits from repurposed medications for addiction treatment?
Answer:
🏢 1. Pharmaceutical Companies (Sometimes)
- If the drug is still under patent, the original manufacturer can profit by:
- Filing a Supplemental New Drug Application (sNDA) to get the addiction treatment indication officially approved.
- Marketing the drug under a new brand name or formulation.
- However, most repurposed drugs are off-patent (generic), offering limited profit opportunities, so many companies choose not to pursue formal approval for addiction use.
🧪 2. Biotech Startups & Niche Pharma
- Some smaller companies acquire rights to old or shelved drugs, then invest in clinical trials to gain new approvals (including for addiction).
- If successful, they can:
- License the drug.
- Sell the company.
- Seek priority review vouchers or grants (like from NIH/NIDA) for future profit leverage.
🏥 3. Contract Research Organizations (CROs) & Trial Networks
- Organizations conducting clinical trials are paid to test these drugs in addiction-related studies.
- They profit indirectly through research grants, partnerships, or data licensing.
🧑⚕️ 4. Health Systems and Addiction Clinics
- Clinics that incorporate repurposed medications into treatment plans may:
- Improve patient retention and outcomes, leading to higher reimbursement rates.
- Offer in-house pharmacy services that benefit from prescription volumes.
📚 5. Academic Institutions
- Universities and researchers may benefit through:
- NIH/NIDA grants to study repurposed drugs.
- Intellectual property rights if they identify a novel use or formulation.
- Consulting or licensing deals if the repurposed drug is later commercialized.
🚫 Who Usually Doesn’t Profit?
- When medications are generic and used off-label, no single company profits directly.
- Clinicians and public addiction programs often use these medications to improve care, not for revenue.
Question: How do clinical trials prove that the medications work for addiction treatment?
Answer:
Clinical trials prove that medications work for addiction treatment by using scientific, ethical, and statistical methods to test whether the drug produces meaningful improvements in people with substance use disorders. Here’s how that process works:
🧪 1. Controlled Study Design
- Randomized Controlled Trials (RCTs) are the gold standard.
- Participants are randomly assigned to receive either the study drug or a placebo (or another treatment).
- This helps eliminate bias and ensures that any observed effects are due to the drug, not to chance or external factors.
🧍♂️🧍♀️ 2. Careful Participant Selection
- Researchers define inclusion/exclusion criteria (e.g., age, type of addiction, co-occurring disorders).
- This ensures the drug is tested in relevant populations while protecting participants’ safety.
🧠 3. Use of Validated Outcome Measures
Researchers track whether the medication improves:
- Cravings (using scales like the Visual Analog Scale for Craving)
- Substance use behavior (through urine drug screens, self-reports, or digital tracking)
- Abstinence or reduction in use
- Relapse rates over time
- Functioning, such as improved sleep, mood, work stability, or reduced ER visits
⏳ 4. Time-Based Monitoring
- Trials often last 8 to 24 weeks or longer to observe short- and medium-term effects.
- Follow-ups may extend beyond the treatment period to measure relapse prevention.
📉 5. Statistical Analysis
- Data are analyzed to determine whether the drug produced statistically significant improvements versus placebo.
- Researchers also calculate effect sizes, response rates, and safety profiles to understand how substantial and safe the benefit is.
⚖️ 6. Safety and Ethics Oversight
- Institutional Review Boards (IRBs) ensure the protection of participants.
- Adverse effects are recorded, and trials can be stopped early if risks outweigh benefits.
🔁 7. Repeated Trials & Peer Review
- A single study isn’t enough—evidence is stronger when:
- Multiple trials replicate the findings
- Results are published in peer-reviewed journals
- Findings are included in systematic reviews or meta-analyses
🟢 Example:
Bupropion + Naltrexone for Methamphetamine Use Disorder
- The combination was tested in a double-blind RCT, with significantly more participants achieving abstinence in both weeks 5–6 and 11–12 than the placebo group.
- These findings led to increased off-label clinical use and further research.
Conclusion
While repurposing medications for addiction treatment holds promise for expanding therapeutic options and accelerating access, it is not without significant hurdles. Scientific, regulatory, and practical challenges must be navigated carefully to ensure safe and effective use. Ethical dilemmas—such as informed consent, equitable access, and treatment integrity—require ongoing attention, particularly when dealing with vulnerable populations. Government involvement remains essential in guiding clinical standards, funding research, and shaping policies that protect patients while fostering innovation. A balanced approach that prioritizes evidence, ethics, and access is key to realizing the full potential of drug repurposing in addiction care.
Video: Are Medications Originally Made for Other Conditions the KEY to Beating Addiction?