During the presidency of George W. Bush (2001–2009), U.S. drug policy largely preserved the traditional War on Drugs structure while gradually broadening attention to treatment, prevention, and community-based services. His administration continued to provide strong federal support for law enforcement and interdiction efforts, while also advancing recovery-oriented measures such as drug courts, youth prevention initiatives, and expanded funding for community- and faith-based treatment programs. Rising concern about methamphetamine use and early prescription opioid misuse prompted both regulatory actions and public education efforts. In essence, Bush’s strategy combined firm enforcement priorities with a growing acknowledgment of addiction as a public health issue requiring wider access to treatment and preventive resources.
President George W. Bush’s Drug Reform Policy: Enforcement, Faith-Based Initiatives, and Treatment Expansion
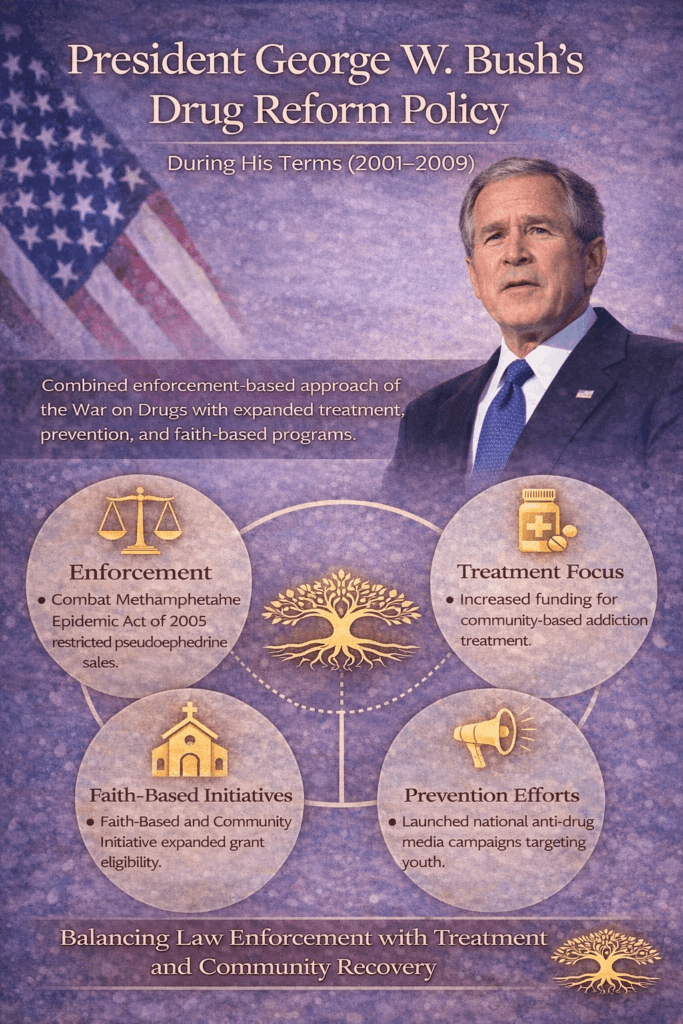
During the presidency of George W. Bush (2001–2009), U.S. drug policy reflected a dual approach: continued enforcement within the War on Drugs framework alongside expanded attention to treatment, prevention, and faith-based recovery initiatives. His administration operated during a time when methamphetamine use was rising nationally, and concerns about prescription drug misuse were increasing.
One of the central themes of Bush’s drug policy was balancing law enforcement with treatment access. While federal funding continued to support interdiction and criminal justice strategies, his administration also promoted community-based prevention programs and recovery-oriented services. The Office of National Drug Control Policy (ONDCP) under his leadership emphasized reducing drug demand through youth prevention campaigns and public education efforts.
A significant feature of Bush’s drug reform approach was the expansion of faith-based and community initiatives. Through the Faith-Based and Community Initiative program, federal funding pathways were broadened to enable religious and grassroots organizations to compete for grants to support addiction treatment and recovery services. This approach aimed to decentralize services and strengthen local recovery ecosystems.
Methamphetamine control became a high priority. The Combat Methamphetamine Epidemic Act of 2005 imposed restrictions on the sale of pseudoephedrine-containing products to reduce domestic meth production. The legislation required identification and purchase limits, reflecting a supply-side regulatory strategy.
Prevention messaging during Bush’s presidency included national anti-drug campaigns targeting youth. These initiatives sought to reduce experimentation rates through media outreach and school-based education. However, critics questioned the measurable long-term effectiveness of some federally funded media campaigns.
The administration also supported drug courts as alternatives to incarceration for nonviolent offenders, emphasizing rehabilitation over purely punitive responses in certain cases. This reflected a gradual evolution of policy toward treatment-involved justice reform.
From a policy perspective, Bush’s drug strategy represented continuity with earlier enforcement-focused frameworks while incorporating expanded recovery and prevention components. The era did not fundamentally dismantle the War on Drugs structure, but it did reinforce community-based treatment access and faith-driven recovery support as legitimate policy tools.
Ultimately, President George W. Bush’s drug reform policies illustrate a transitional phase in U.S. addiction policy—maintaining strong enforcement measures while gradually increasing recognition of treatment, recovery, and prevention as essential components of national drug strategy.
Advantages of President George W. Bush’s Drug Reform Policy: Expanding Treatment While Strengthening Enforcement
During the administration of George W. Bush, U.S. drug policy combined continued enforcement efforts with expanded support for treatment, prevention, and community-based recovery initiatives. While the broader War on Drugs framework remained intact, several advantages emerged from the policy direction taken during his terms (2001–2009).
One major advantage was the increased emphasis on treatment accessibility. The Bush administration supported expanded funding for substance use treatment programs, particularly through community and faith-based organizations. By broadening eligibility for federal grants, smaller grassroots organizations were able to compete for funding, increasing the diversity of treatment providers and strengthening local recovery networks. This decentralization allowed communities to tailor services to their specific populations.
Another key strength was the formal recognition of recovery as a long-term process. The administration promoted recovery-oriented messaging and helped elevate public awareness that addiction is not solely a criminal justice issue but also a public health concern. Drug courts, which divert nonviolent offenders into structured treatment programs instead of incarceration, gained continued support during this period. These courts demonstrated improved outcomes in reducing recidivism and promoting rehabilitation.
The Combat Methamphetamine Epidemic Act of 2005 represented a targeted regulatory success. By restricting over-the-counter sales of pseudoephedrine-containing products, the law significantly reduced domestic methamphetamine production in the short term. This legislation reflected an evidence-informed supply control strategy aimed at limiting access to precursor chemicals.
Youth prevention campaigns were also a priority. National media initiatives sought to decrease experimentation among adolescents through public education and school-based prevention messaging. Although debates continue about long-term effectiveness, the advantage lies in elevating prevention as a visible national concern.
Additionally, integrating faith-based and community initiatives expanded engagement among populations that may have distrusted traditional government systems. Many individuals in recovery found culturally aligned support within these community-driven programs.
From a systems perspective, Bush’s drug reform policies maintained enforcement infrastructure while gradually strengthening treatment and prevention capacity. The dual focus acknowledged the complexity of addiction and reinforced the idea that sustainable solutions require both accountability and rehabilitation.
Overall, the advantages of President George W. Bush’s drug reform policy included expanded community involvement, increased treatment access, targeted methamphetamine control, continued support for drug courts, and heightened national attention to prevention and recovery.
Disadvantages of President George W. Bush’s Drug Reform Policy: Limits of a Dual Enforcement–Treatment Approach
During the presidency of George W. Bush (2001–2009), federal drug policy maintained a strong enforcement framework while expanding treatment and prevention initiatives. Although the administration supported community-based recovery and targeted methamphetamine production, several limitations and criticisms emerged.
One primary disadvantage was the continued reliance on the broader War on Drugs model. Federal funding remained heavily weighted toward interdiction, law enforcement, and incarceration rather than comprehensive public health reform. Critics argued that this approach sustained high incarceration rates for nonviolent drug offenses and contributed to long-term social and economic disparities, particularly in marginalized communities.
While treatment funding increased in certain areas, access gaps persisted. Rural communities and underserved populations continued to face shortages of qualified addiction treatment providers. The emphasis on faith-based initiatives expanded service options, but some critics questioned whether all funded programs consistently met standardized evidence-based practice benchmarks.
The national anti-drug media campaigns launched during this era also drew scrutiny. Independent evaluations suggested limited measurable impact on long-term substance use trends among youth, raising concerns about cost-effectiveness relative to other prevention strategies.
The Combat Methamphetamine Epidemic Act of 2005 successfully reduced domestic meth production in the short term; however, critics note that production shifted internationally, particularly to large-scale operations outside the United States. As a result, domestic supply disruptions did not eliminate long-term availability.
Additionally, the administration did not substantially reform federal sentencing laws related to drug offenses. Mandatory minimum sentencing policies remained largely intact during this period, limiting judicial discretion and contributing to prison overcrowding.
Another limitation involved insufficient focus on emerging prescription opioid misuse, which was escalating during the early 2000s. Although prevention messaging existed, comprehensive opioid-specific reforms were not fully developed before the broader opioid crisis intensified later.
From a policy perspective, the Bush administration represented continuity rather than structural transformation. While incremental improvements occurred in treatment and community engagement, systemic criminal justice reform and large-scale public health restructuring were limited.
Overall, the disadvantages of President George W. Bush’s drug reform policy centered on sustained enforcement dominance, uneven treatment access, questions about prevention campaign effectiveness, limited sentencing reform, and delayed response to emerging prescription drug trends.
Ethical Dilemmas in President George W. Bush’s Drug Reform Policy: Balancing Enforcement, Faith, and Public Health
During the administration of George W. Bush (2001–2009), federal drug policy reflected a dual emphasis on law enforcement and expanded treatment initiatives. While this approach aimed to address both supply and demand, it also raised several ethical dilemmas concerning justice, public health priorities, religious involvement in government funding, and the proportionality of punishment.
One central ethical tension involved the continued prioritization of enforcement within the broader War on Drugs framework. Although treatment and prevention funding increased, federal expenditures remained heavily directed toward interdiction and incarceration. Critics questioned whether punitive approaches aligned with emerging evidence recognizing addiction as a chronic medical condition. The ethical dilemma centered on proportionality: Should substance use disorders be treated primarily as criminal behavior or as health conditions requiring therapeutic intervention?
Another ethical concern was mandatory minimum sentencing laws, which remained largely intact during this period. While drug courts and diversion programs expanded, sentencing disparities and prison overcrowding persisted. This raised justice-based questions about equity, particularly regarding the disproportionate impact of drug enforcement policies on marginalized communities.
Faith-based funding initiatives also generated ethical debate. The Bush administration expanded access to federal grants for religious and community organizations that provide addiction services. Supporters viewed this as empowering local recovery networks; critics questioned whether government funding could be ethically separated from religious influence. The tension involved maintaining constitutional boundaries while respecting community-based recovery models.
The Combat Methamphetamine Epidemic Act of 2005 introduced restrictions on over-the-counter medications containing pseudoephedrine. While designed to reduce domestic meth production, it raised ethical considerations about balancing public safety with consumer access and personal freedom. Limiting access to common cold medications for the broader population in response to criminal misuse illustrated the tension between collective protection and individual rights.
Prevention media campaigns also presented ethical questions about evidence-based spending. Critics argued that federally funded youth campaigns should demonstrate measurable outcomes proportional to their cost, emphasizing stewardship of public resources.
From a public health ethics perspective, another concern involved the early stages of prescription opioid escalation. Some argue that broader structural reforms and stronger regulatory oversight might have mitigated emerging risks earlier.
Overall, the ethical dilemmas of President George W. Bush’s drug reform policy reflected a transitional period in U.S. drug governance. The administration attempted to balance enforcement, community empowerment, and treatment expansion—but tensions between punishment and rehabilitation, religious inclusion and neutrality, and security and liberty remained central to policy debates.
Frequently Asked Questions
Here are some common questions:
1. What was the overall focus of President George W. Bush’s drug policy?
During the administration of George W. Bush, drug policy maintained a strong enforcement foundation while expanding treatment, prevention, and faith-based recovery initiatives. His approach reflected continuity with the War on Drugs framework while incorporating greater community-level engagement.
2. Did President Bush support treatment programs?
Yes. His administration increased funding for community-based addiction treatment programs and supported recovery-oriented initiatives. Faith-based and grassroots organizations were given expanded access to federal grants to deliver addiction services.
3. What was the Combat Methamphetamine Epidemic Act of 2005?
The Combat Methamphetamine Epidemic Act restricted over-the-counter sales of products containing pseudoephedrine, a key ingredient used in methamphetamine production. The goal was to reduce domestic meth labs and limit supply.
4. How did Bush’s administration address prevention?
The administration funded national anti-drug media campaigns targeting youth and supported school-based prevention programs. These efforts aimed to reduce early experimentation and drug initiation rates.
5. Were drug courts supported during his presidency?
Yes. Drug courts, which divert nonviolent offenders into supervised treatment programs rather than incarceration, continued to receive support. These courts were seen as a way to combine accountability with rehabilitation.
6. What role did faith-based organizations play?
Through the Faith-Based and Community Initiative, religious and local organizations were allowed to compete for federal funding to provide addiction treatment and recovery services. This expanded community participation in federal drug policy efforts.
7. Was enforcement still a major component?
Yes. Federal funding remained heavily directed toward law enforcement, interdiction, and criminal justice strategies. The broader War on Drugs framework was not dismantled during this period.
8. Did Bush’s policies address the opioid crisis?
Prescription opioid misuse was emerging during the early 2000s, but comprehensive opioid-specific reforms were not fully developed before the crisis escalated in later years.
9. What were common criticisms of his drug policy?
Critics cited continued reliance on incarceration, limited sentencing reform, and questions about the effectiveness of national media prevention campaigns. Others raised concerns about disparities within enforcement outcomes.
10. How is Bush’s drug reform policy viewed historically?
His administration is often seen as a transitional phase in U.S. drug policy—maintaining strong enforcement while gradually increasing recognition of treatment, recovery, and community-based strategies as essential components of national drug control efforts.
Conclusion
President George W. Bush’s drug reform policy illustrates a transitional chapter in American addiction policy. While enforcement structures remained prominent, the administration expanded access to treatment, strengthened drug court alternatives, and elevated prevention messaging at the national level. The era did not fundamentally dismantle punitive frameworks, but it did signal growing acknowledgment that recovery, community engagement, and prevention are essential components of long-term drug policy strategy. Ultimately, Bush’s approach reflected the ongoing national effort to balance criminal justice priorities with public health considerations—an evolving debate that continues to shape addiction policy today.
Video: Why Bush Did Treatment Instead of Prison #drugpolicy #shorts