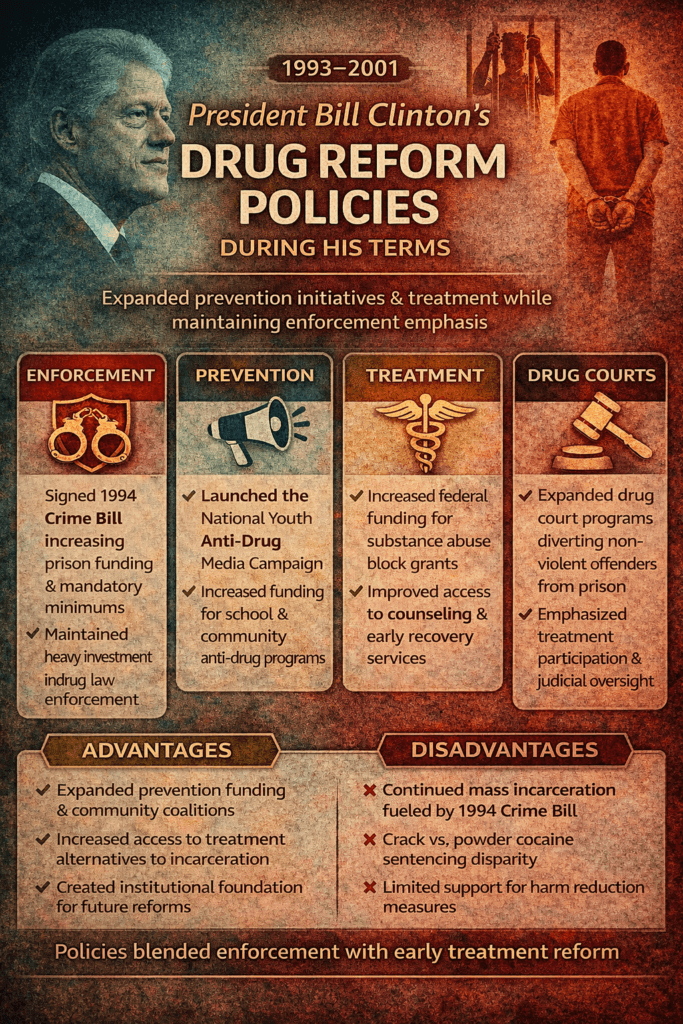
During the presidency of Bill Clinton (1993–2001), U.S. drug policy operated at a crossroads between traditional “War on Drugs” enforcement strategies and emerging public health–oriented reforms. His administration maintained strong law enforcement funding and supported legislation such as the 1994 Violent Crime Control and Law Enforcement Act, which influenced drug-related sentencing and incarceration trends. At the same time, Clinton expanded prevention initiatives, strengthened community anti-drug coalitions, increased treatment block grants to states, and supported the growth of drug courts as alternatives to incarceration. This dual approach reflected the political and social climate of the 1990s, balancing public safety concerns with growing recognition of addiction as a medical and social issue.
President Bill Clinton’s Drug Reform Policies During His Terms
During the presidency of Bill Clinton (1993–2001), U.S. drug policy reflected a complex blend of enforcement expansion, prevention investment, and early steps toward treatment reform. His administration operated during a transitional period in American drug policy—still heavily influenced by the “War on Drugs” framework of the 1980s, yet increasingly aware of addiction as a public health issue. Clinton’s approach combined law enforcement measures with growing support for prevention programming and treatment access.
Continuation of the War on Drugs Framework
Clinton did not dismantle the War on Drugs structure established under previous administrations. Federal funding for drug enforcement remained substantial, and policies supporting incarceration for drug offenses continued. The 1994 Violent Crime Control and Law Enforcement Act expanded prison funding and reinforced mandatory minimum sentencing policies that disproportionately affected drug-related offenses.
While framed as a broader crime bill, it significantly influenced drug enforcement practices by increasing law enforcement resources and prison construction nationwide.
Expansion of Prevention Programs
One of Clinton’s major drug policy initiatives was investment in prevention. The administration launched the National Youth Anti-Drug Media Campaign in 1998, designed to reduce youth drug use through public service advertising. Billions of dollars were allocated to school-based prevention efforts and community coalitions to reduce early substance experimentation.
This marked a shift toward recognizing the importance of early intervention and community-level prevention strategies rather than focusing solely on criminal justice responses.
Growth in Treatment Funding
Clinton’s administration increased federal funding for substance use treatment, including block grants to states through the Substance Abuse and Mental Health Administration’s (SAMHSA) Substance Abuse Prevention and Treatment (SAPT) Block Grant. There was also expanded support for drug courts, which provided supervised treatment alternatives to incarceration for nonviolent drug offenders. Drug courts became a significant structural reform during the 1990s, integrating accountability with rehabilitation.
While medication-assisted treatment (MAT) was not as widely implemented as in later decades, the groundwork for integrating treatment into public systems continued to develop during this period.
Crack vs. Powder Cocaine Sentencing Debate
One of the most controversial aspects of the 1990s drug policy was the sentencing disparity between crack and powder cocaine offenses. Clinton signed legislation that maintained the 100-to-1 sentencing disparity, despite criticism from civil rights advocates who argued it disproportionately impacted Black communities. Although there were discussions about reform, meaningful federal sentencing adjustments did not occur until later administrations.
Public Health vs. Criminal Justice Balance
Clinton’s drug policy reflected tension between public health and criminal justice approaches. On the one hand, funding for prevention and treatment increased. On the other hand, incarceration rates for drug-related offenses continued to rise during much of the 1990s. The administration’s stance demonstrated incremental reform within a largely enforcement-driven national framework.
Long-Term Impact
Clinton’s drug policies influenced decades of criminal justice and addiction treatment systems. The expansion of drug courts and prevention campaigns laid the groundwork for more balanced approaches. However, the continued reliance on incarceration contributed to long-term prison population growth and disparities that later administrations sought to address.
Conclusion
President Bill Clinton’s drug reform policies represented a hybrid era in U.S. drug policy—maintaining enforcement-driven strategies while increasing attention to prevention and treatment. His administration did not fundamentally shift away from the War on Drugs model, but it expanded community prevention efforts and treatment alternatives that helped shape later public health–oriented reforms. The legacy of this period remains central to ongoing debates about accountability, sentencing reform, and the balance between public safety and addiction treatment.
The Advantages of President Bill Clinton’s Drug Reform Policies
During Bill Clinton’s presidency (1993–2001), U.S. drug policy maintained elements of enforcement while expanding prevention and treatment initiatives. Although often debated, several advantages emerged from the administration’s approach. Clinton’s policies reflected an era of transition—preserving public safety priorities while increasing investment in community-based prevention and alternative sentencing.
1. Expansion of Drug Courts
One of the most significant advantages of Clinton-era reforms was the expansion of drug courts nationwide. These courts diverted nonviolent drug offenders into supervised treatment rather than traditional incarceration. Drug courts emphasized accountability, mandatory treatment participation, and judicial oversight. This model improved treatment engagement rates and helped establish a framework that integrated rehabilitation with structured consequences.
Drug courts became a foundational component of modern recovery-oriented justice systems.
2. Increased Investment in Prevention
The administration significantly expanded prevention funding, including the National Youth Anti-Drug Media Campaign and community-based coalitions. By focusing on early intervention, school-based programming, and public awareness efforts, the government aimed to reduce initiation of drug use among adolescents.
Prevention initiatives contributed to declining youth drug use trends in certain categories during the late 1990s, reflecting the benefit of coordinated public messaging and education strategies.
3. Strengthening Community Coalitions
Clinton’s policies supported community-driven anti-drug coalitions that allowed local leaders, schools, healthcare providers, and law enforcement to collaborate. This decentralized approach empowered communities to tailor prevention strategies to local needs rather than relying solely on federal mandates.
Community engagement strengthened public health infrastructure and fostered shared responsibility.
4. Increased Treatment Funding
Federal funding for substance use treatment increased during Clinton’s terms through block grants to states. While not yet fully aligned with today’s medication-assisted treatment standards, these investments improved access to counseling, outpatient programs, and early recovery services.
By reinforcing treatment as a necessary component of drug policy, the administration helped shift some national dialogue toward recognizing addiction as a health condition rather than solely a criminal issue.
5. Balancing Accountability with Rehabilitation
Clinton’s era maintained a focus on law enforcement while simultaneously expanding structured alternatives. This hybrid approach reinforced accountability while beginning to normalize treatment diversion programs. The expansion of supervised rehabilitation programs created a policy bridge between punitive models and modern recovery-oriented systems.
6. Institutional Foundation for Later Reforms
While not fully reformative by contemporary standards, Clinton’s policies laid the groundwork for future sentencing reforms and public health–centered approaches. The institutionalization of drug courts, expanded prevention programming, and treatment funding created an infrastructure that later administrations would build upon when advancing opioid response initiatives and sentencing reforms.
Conclusion
The advantages of President Bill Clinton’s drug reform policies lie primarily in their expansion of prevention, community coalitions, treatment funding, and drug court systems. Although enforcement remained central, the administration introduced structural elements that integrated rehabilitation into the national drug strategy. These efforts helped establish frameworks that continue to influence modern addiction policy, blending accountability with access to care and community-based prevention.
The Disadvantages of President Bill Clinton’s Drug Reform Policies
During the presidency of Bill Clinton, U.S. drug policy continued many enforcement-driven strategies established during earlier phases of the War on Drugs. While his administration expanded prevention programs and drug courts, several disadvantages emerged from policies enacted during this period. Critics argue that aspects of Clinton-era reforms contributed to mass incarceration, racial disparities, and long-term structural challenges in addiction policy.
1. Expansion of Mass Incarceration
One of the most frequently cited concerns relates to the 1994 Violent Crime Control and Law Enforcement Act. Although broader than drug policy alone, it significantly increased prison funding and reinforced sentencing structures that affected drug offenses. The expansion of incarceration capacity contributed to rising prison populations throughout the 1990s.
Mandatory minimum sentencing laws—many established earlier but maintained during Clinton’s presidency—continued to impose lengthy sentences for nonviolent drug offenses. Critics argue that this approach prioritizes punishment over rehabilitation.
2. Crack vs. Powder Cocaine Sentencing Disparity
During Clinton’s terms, the federal 100-to-1 sentencing disparity between crack and powder cocaine remained intact. Under this structure, possession of crack cocaine triggered significantly harsher penalties than powder cocaine offenses. Research and civil rights advocates later highlighted that this disparity disproportionately affected Black communities.
Although discussions about reform occurred, significant sentencing adjustments did not materialize until later administrations, leaving Clinton-era policies associated with persistent inequities.
3. Continued Emphasis on Enforcement
Despite growth in prevention and treatment funding, enforcement spending remained substantial. Law enforcement expansion sometimes overshadowed public health initiatives. Critics argue that this imbalance delayed broader adoption of harm reduction strategies and medication-assisted treatment models that would later become central in opioid use disorder care.
The continued framing of addiction through a criminal justice lens may have reinforced stigma and discouraged treatment-seeking behaviors.
4. Limited Advancement of Harm Reduction
During the 1990s, harm reduction strategies such as needle exchange programs faced federal funding restrictions. While some local initiatives emerged, national policy support was limited. This constraint likely slowed the expansion of evidence-based interventions aimed at reducing HIV transmission and overdose risk among people who inject drugs.
5. Collateral Consequences for Individuals and Families
Drug-related convictions during this era carried long-term collateral consequences, including barriers to employment, housing, education funding, and public benefits. These restrictions contributed to cycles of poverty and instability, which are known risk factors for relapse and recidivism.
Communities already experiencing economic hardship were disproportionately affected.
6. Delayed Shift Toward Public Health Framing
Although prevention programs expanded, addiction was not yet fully embraced as a chronic medical condition requiring integrated healthcare treatment. The broader transformation toward public health–oriented addiction policy would accelerate more significantly in later decades, particularly during the opioid epidemic.
Conclusion
The disadvantages of President Bill Clinton’s drug reform policies center on the continuation and expansion of incarceration-based strategies, maintenance of sentencing disparities, limited harm reduction support, and long-term collateral consequences for affected communities. While prevention and treatment investments were meaningful, enforcement remained dominant in shaping national drug policy during this period. The legacy of these decisions continues to inform contemporary debates about sentencing reform, racial equity, and the balance between criminal justice and public health approaches to addiction.
The Ethical Dilemmas of President Bill Clinton’s Drug Reform Policies
During Bill Clinton’s presidency, U.S. drug policy reflected a transitional period between the strict enforcement models of the 1980s and the emerging public health frameworks that would expand in later decades. While his administration increased prevention funding and expanded drug courts, it also upheld incarceration-driven strategies and controversial sentencing laws. These dual approaches created significant ethical dilemmas involving justice, equity, public safety, and medical responsibility.
1. Punishment vs. Public Health
One of the central ethical tensions involved the balance between criminal justice enforcement and treatment-based care. Addiction is now widely recognized as a chronic medical condition affecting brain function and behavior. However, during the 1990s, federal drug policy still heavily emphasized incarceration for nonviolent drug offenses.
The ethical question arises: should individuals with substance use disorders be treated primarily as offenders or as patients? While Clinton expanded prevention and drug courts, enforcement remained dominant, raising concerns about whether punishment overshadowed medical compassion.
2. The Crack vs. Powder Cocaine Sentencing Disparity
The continuation of the 100-to-1 sentencing disparity between crack and powder cocaine offenses presented a major ethical challenge. Because crack cocaine was more prevalent in urban, predominantly Black communities, the sentencing structure resulted in disproportionate incarceration rates among minority populations.
This disparity raised issues of distributive justice and racial equity. Although there were debates about reform, the policy remained largely unchanged during Clinton’s presidency, which intensified concerns about fairness and systemic bias.
3. Mass Incarceration and Social Consequences
The 1994 Violent Crime Control and Law Enforcement Act increased prison capacity and reinforced sentencing structures. While intended to address rising crime rates, it contributed to the expanded incarceration of individuals for drug-related offenses.
Ethically, this raises questions about proportionality and long-term societal harm. Incarceration carries collateral consequences—including employment barriers, housing instability, and family disruption—that may perpetuate cycles of poverty and addiction.
4. Harm Reduction Restrictions
During the 1990s, federal funding limitations on needle exchange programs limited the expansion of harm reduction. At a time when HIV transmission among people who inject drugs was a significant public health concern, limitations on harm reduction created ethical tension between political caution and evidence-based disease prevention.
The ethical dilemma centered on whether reducing harm should take precedence over concerns that such programs might appear to condone drug use.
5. Balancing Accountability with Compassion
Clinton’s expansion of drug courts attempted to bridge accountability and rehabilitation. Drug courts required structured treatment participation while offering alternatives to incarceration. Ethically, this model reflected an effort to combine responsibility with care.
However, critics questioned whether coercive treatment under judicial supervision fully respected patient autonomy or was a necessary compromise in the criminal justice context.
Conclusion
The ethical dilemmas of President Bill Clinton’s drug reform policies reflect the complexity of governing during a transitional era in addiction policy. His administration expanded prevention, treatment funding, and drug courts, yet maintained enforcement-heavy strategies and sentencing disparities that contributed to long-term inequities. The tension between punishment and public health, equity and enforcement, autonomy and accountability remains central in contemporary addiction policy debates. Examining these dilemmas provides valuable insight into how ethical considerations shape the balance between justice, compassion, and public safety in drug reform.
Frequently Asked Questions
Here are some common questions:
1. When did Bill Clinton serve as president?
Bill Clinton served as the 42nd President of the United States from 1993 to 2001.
2. What was the overall approach of Clinton’s drug policy?
Clinton’s drug policy blended continued emphasis on law enforcement with expanded prevention and treatment initiatives. His administration maintained aspects of the War on Drugs framework while increasing funding for prevention campaigns and drug courts.
3. What was the 1994 Crime Bill, and how did it affect drug policy?
The 1994 Violent Crime Control and Law Enforcement Act increased prison funding and supported tougher sentencing measures. Although broader than drug policy alone, it contributed to expanded incarceration for drug-related offenses.
4. Did Clinton expand drug treatment programs?
Yes. His administration increased federal funding for substance abuse treatment through block grants to states and supported the growth of drug courts, which diverted nonviolent drug offenders into supervised treatment instead of prison.
5. What were drug courts, and why were they significant?
Drug courts provided structured alternatives to incarceration by requiring offenders to participate in treatment programs under judicial supervision. This model integrated accountability with rehabilitation and became a lasting feature of U.S. addiction policy.
6. What was the crack vs. powder cocaine sentencing issue?
During Clinton’s presidency, the federal 100-to-1 sentencing disparity between crack and powder cocaine offenses remained in place. Critics argued that the policy disproportionately impacted Black communities and raised concerns about racial equity.
7. Did Clinton support prevention efforts?
Yes. The administration launched the National Youth Anti-Drug Media Campaign and increased funding for school- and community-based prevention programs aimed at reducing youth drug use.
8. How did his policies affect incarceration rates?
Incarceration rates for drug-related offenses remained high during the 1990s. While drug courts expanded treatment options, enforcement policies, and sentencing structures contributed to continued growth in prison populations.
9. Was harm reduction emphasized during his terms?
Harm reduction strategies, such as federally funded needle exchange programs, received limited support during the 1990s due to federal restrictions. This reflected ongoing political and public health debates of the time.
10. How are Clinton’s drug policies viewed today?
Clinton’s drug policies are often viewed as transitional. Supporters highlight expanded prevention and treatment infrastructure, particularly drug courts. Critics focus on mass incarceration trends and sentencing disparities. His administration laid the groundwork for later reforms while remaining largely enforcement-driven.
Conclusion
President Clinton’s drug reform policies represent a transitional era in American addiction policy. While enforcement and incarceration remained central features, the expansion of prevention programs, treatment funding, and drug courts laid the structural groundwork for later reforms that would increasingly frame addiction as a public health condition. The legacy of this period continues to influence contemporary debates about sentencing reform, racial equity, accountability, and access to treatment. Evaluating his policies highlights the ongoing challenge of balancing justice, public safety, and compassionate care within national drug policy frameworks.
Video: Bill Clinton Proved Both Enforcement AND Treatment Work Together #DrugPolicy #Reform